
Beta-Sitosterol is a plant sterol (phytosterol) with a chemical structure similar to cholesterol, found in a variety of plant-based foods such as nuts, seeds, vegetables, and fruits. As one of the most abundant phytosterols, it is widely recognized for its potential to lower cholesterol levels, support prostate health, and provide anti-inflammatory and antioxidant benefits. Used traditionally in herbal medicine and now as a dietary supplement, Beta-Sitosterol is incorporated into functional foods, capsules, and topical preparations. Modern research supports its efficacy in managing hypercholesterolemia and benign prostatic hyperplasia (BPH), though its benefits for other conditions are less established. This article explores Beta-Sitosterol’s chemical characteristics, sources, historical and contemporary uses, pharmacological properties, clinical evidence, side effects, and practical applications.
Chemical Characteristics and Sources
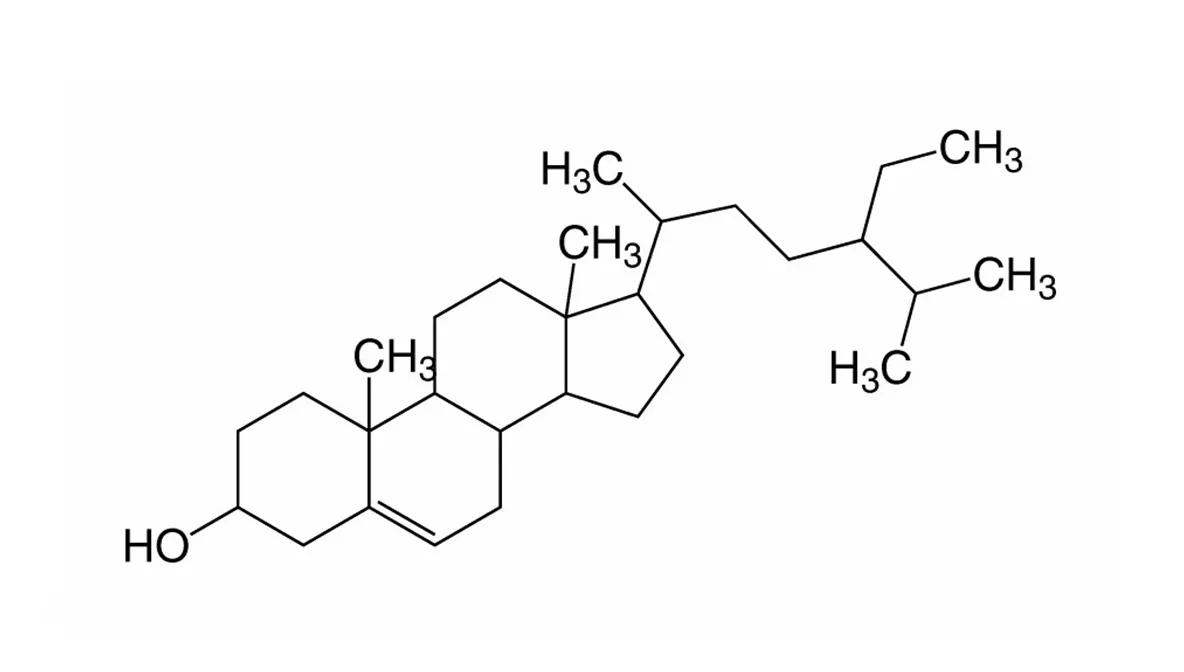
Beta-Sitosterol is a naturally occurring sterol with distinct chemical and biological properties:
- Chemical Structure: A steroidal compound (C₂₉H₅₀O) with a structure analogous to cholesterol, featuring a sterol nucleus and a hydroxyl group, differing by an ethyl group at C-24.
- Physical Properties: White, waxy, fat-soluble powder, insoluble in water, stable under heat and light.
- Natural Sources:
- Nuts and Seeds: Almonds, pistachios, pumpkin seeds, and sesame seeds (10–400 mg/100 g).
- Oils: Corn oil, soybean oil, and wheat germ oil (100–900 mg/100 g).
- Fruits and Vegetables: Avocados, sea buckthorn, and corn (10–90 mg/100 g).
- Grains and Legumes: Wheat germ, rice bran, and soybeans (50–200 mg/100 g).
- Herbs: Saw palmetto and pygeum, used in prostate health supplements, are rich in Beta-Sitosterol.
- Commercial Forms: Extracted from soybeans, pine bark, or sugarcane pulp, available as supplements (capsules, tablets, powders) standardized to 60–90% Beta-Sitosterol, often combined with other phytosterols (campesterol, stigmasterol).
Dietary intake in Western diets is typically 100–300 mg/day, far below therapeutic doses (1.5–3 g/day).
Historical and Traditional Uses
Beta-Sitosterol has a history rooted in traditional medicine, though its identification as a distinct compound is relatively recent:
- Traditional Medicine: Plants rich in phytosterols, like saw palmetto and pumpkin seeds, were used in Native American, African, and European herbalism for urinary and reproductive issues, particularly in men. Beta-Sitosterol was likely an active component.
- Ayurveda and TCM: Seeds and oils (e.g., sesame, wheat germ) were used for vitality, digestion, and skin health, indirectly providing Beta-Sitosterol.
- Modern Discovery: Isolated in the 1920s, Beta-Sitosterol gained attention in the 1950s for cholesterol-lowering effects, leading to its use in functional foods (e.g., margarine) and supplements.
- Historical Context: In the 19th century, phytosterol-rich remedies were prescribed for heart health and inflammation, though without specific knowledge of Beta-Sitosterol.
Traditional preparations included seed decoctions, oils, or poultices, while modern uses focus on concentrated extracts.
Nutritional and Chemical Composition
Beta-Sitosterol is not a nutrient but a bioactive compound with no caloric value:
- Purity in Supplements: Typically 60–90% Beta-Sitosterol, with campesterol, stigmasterol, and minor sterols as co-components.
- Associated Compounds: In natural sources, accompanied by fatty acids (e.g., linoleic acid), tocopherols, and polyphenols, enhancing bioavailability and antioxidant effects.
- Dietary Contribution: Provides no vitamins, minerals, or macronutrients but contributes to cholesterol absorption inhibition when consumed in therapeutic amounts.
- Bioavailability: Poorly absorbed (5–10% in the gut), with most exerting local effects in the intestines before excretion. Esterification (e.g., sitosterol esters) improves absorption in functional foods.
Pharmacological Mechanisms
Beta-Sitosterol’s effects are driven by its structural similarity to cholesterol and anti-inflammatory properties, supported by preclinical and clinical studies:
- Cholesterol Reduction: Competes with dietary and biliary cholesterol for micellar incorporation in the gut, reducing cholesterol absorption by 30–50%. Increases LDL receptor expression in the liver, enhancing cholesterol clearance.
- Anti-inflammatory Effects: Inhibits pro-inflammatory cytokines (e.g., TNF-α, IL-6) and enzymes (e.g., COX-2), reducing systemic and localized inflammation.
- Prostate Health: Modulates androgen metabolism, inhibits 5-alpha-reductase (converting testosterone to DHT), and reduces prostate cell proliferation, alleviating BPH symptoms.
- Antioxidant Activity: Scavenges free radicals and upregulates antioxidant enzymes (e.g., superoxide dismutase), protecting against oxidative stress.
- Immunomodulation: Enhances T-cell and NK cell activity, potentially supporting immune responses, though evidence is preliminary.
- Anticancer Potential: Inhibits cancer cell proliferation (e.g., prostate, breast) in vitro by inducing apoptosis and cell cycle arrest, though human data are lacking.
These mechanisms make Beta-Sitosterol a candidate for cardiovascular, urological, and inflammatory conditions.
Potential Benefits
Beta-Sitosterol has been studied for several health benefits, with stronger evidence for cholesterol and prostate health:
1. Cholesterol Reduction
- A 2019 meta-analysis (50 RCTs, >4000 participants) found Beta-Sitosterol (1.5–3 g/day) reduced LDL cholesterol by 0.3–0.5 mmol/L (8–12%), with no significant effect on HDL or triglycerides. Effects were dose-dependent and sustained over 6–12 months.
- A 2020 study showed additive benefits when combined with statins, reducing LDL further than statins alone.
2. Benign Prostatic Hyperplasia (BPH)
- A 2000 meta-analysis (4 RCTs, 519 men) found Beta-Sitosterol (60–195 mg/day) improved BPH symptoms (e.g., urinary flow, residual volume) by 35–50% compared to placebo, with no effect on prostate size.
- A 2016 trial confirmed reduced International Prostate Symptom Score (IPSS) with 130 mg/day, comparable to alpha-blockers in mild cases.
3. Anti-inflammatory Effects
- Preclinical studies show reduced inflammation in arthritis and colitis models, attributed to cytokine suppression.
- A 2017 human study (100 mg/day) reported modest reductions in C-reactive protein (CRP) in hypercholesterolemic patients, but data are limited.
4. Other Potential Benefits
- Immune Support: Small trials suggest enhanced immune response to vaccines, but evidence is inconsistent.
- Anticancer: In vitro studies show inhibition of prostate, breast, and colon cancer cells, but no clinical trials confirm efficacy.
- Hair Loss: Anecdotal use in androgenetic alopecia (combined with saw palmetto), but no robust RCTs.
- Antioxidant Effects: May protect against oxidative stress in cardiovascular disease, though human data are sparse.
Clinical Evidence
Beta-Sitosterol’s evidence base is robust for cholesterol and BPH but weaker for other uses:
- Cholesterol: Meta-analyses (e.g., 2019) confirm consistent LDL reductions, with 2–3 g/day optimal. Effects are smaller than statins but additive.
- BPH: RCTs (e.g., 2000) support symptomatic relief, though not prostate size reduction. Long-term data (>1 year) are limited.
- Other Areas: Anti-inflammatory, immune, and anticancer effects rely on preclinical or small human studies, lacking large-scale RCTs.
Limitations include variability in phytosterol composition (Beta-Sitosterol vs. mixed sterols), short study durations (6–52 weeks), and few comparisons to standard therapies. Most studies use 60–3000 mg/day, with 1.5–3 g/day for cholesterol and 60–130 mg/day for BPH.
Side Effects and Safety
Beta-Sitosterol is generally safe at recommended doses, with a long history of dietary consumption:
- Common: Mild gastrointestinal upset (nausea, bloating, diarrhea), typically dose-dependent.
- Rare: Allergic reactions (rash, itching) or reduced libido (in BPH studies, <1% incidence).
- High Doses: Potential for reduced absorption of fat-soluble vitamins (e.g., vitamin E, beta-carotene), though fortification mitigates this in functional foods.
Contraindications and Interactions
- Drug Interactions: May enhance cholesterol-lowering drugs (e.g., statins, ezetimibe), requiring dose adjustments. Minimal interaction with other medications.
- Sitosterolemia: Contraindicated in this rare genetic disorder, where phytosterols accumulate, increasing cardiovascular risk.
- Pregnancy/Breastfeeding: Insufficient safety data; avoid high-dose supplements unless prescribed.
- Allergies: Avoid in those allergic to soy or other Beta-Sitosterol sources.
- Prostate Cancer: Consult a doctor, as hormonal effects are unclear in prostate cancer patients.
The FDA recognizes phytosterols as GRAS (Generally Recognized as Safe) for food use, with a health claim for cholesterol reduction at 1.3–3.4 g/day. Choose third-party-tested supplements to ensure purity.
Dosage and Administration
- Cholesterol Reduction: 1.5–3 g/day (divided into 2–3 doses), taken with meals to maximize cholesterol competition. Functional foods (e.g., margarine, orange juice) provide 0.8–2 g/serving.
- BPH: 60–130 mg/day (divided doses), often combined with saw palmetto or pygeum.
- Forms: Capsules, tablets, powders, or fortified foods (e.g., spreads, yogurts). Esterified forms (sitosterol esters) are common in foods for better solubility.
- Timing: Effects on cholesterol appear within 2–4 weeks; BPH benefits may take 4–12 weeks. Consistent use is needed for sustained effects.
- Storage: Store supplements in a cool, dry place, away from light to maintain stability.
Practical Applications
- Supplements: Capsules or tablets for cholesterol or BPH management, often combined with other phytosterols or herbs (e.g., saw palmetto). Brands like NOW Foods or Nature’s Way offer standardized products.
- Functional Foods: Fortified margarines (e.g., Benecol), orange juices, or yogurts for daily cholesterol support, ideal for dietary integration.
- Dietary Approach: Increase intake of Beta-Sitosterol-rich foods (e.g., avocados, nuts, seeds) alongside supplements for synergistic effects.
- Topical Use: Emerging in cosmetics for anti-inflammatory and skin barrier benefits, though evidence is limited.
- Considerations: Consult a healthcare provider for BPH, sitosterolemia, or concurrent cholesterol medications.
Recent X posts (as of May 25, 2025) highlight Beta-Sitosterol for prostate health and cholesterol control, with users noting improved urinary flow but occasional digestive upset. Some recommend combining with dietary changes for best results.
Current Research and Future Directions
Beta-Sitosterol research is well-established for cholesterol and BPH but expanding:
- Larger Trials: Needed for anti-inflammatory, immune, and anticancer effects, with comparisons to standard therapies.
- Mechanisms: Clarifying Beta-Sitosterol’s role in androgen metabolism and immune modulation.
- Safety: Long-term studies (>1 year) to assess vitamin absorption and rare conditions like sitosterolemia.
- Bioavailability: Developing formulations (e.g., nanoemulsions) to enhance absorption beyond esterification.
- New Applications: Exploring roles in hair loss, skin health, and metabolic syndrome.
Conclusion
Beta-Sitosterol is a versatile plant sterol with a strong evidence base for lowering LDL cholesterol and alleviating BPH symptoms. Found in nuts, seeds, and oils, it is widely available as a supplement or in functional foods, offering a natural approach to cardiovascular and prostate health. Its anti-inflammatory and antioxidant properties show promise for broader applications, though further research is needed. Safe for most at recommended doses, Beta-Sitosterol requires caution in sitosterolemia and with certain medications. Choosing third-party-tested products ensures quality. As research advances, Beta-Sitosterol may find new roles in integrative health, supported by its long history and modern validation.
References
- AbuMweis, S. S., et al. (2019). European Journal of Clinical Nutrition, 73(6), 805–815.
- Wilt, T. J., et al. (2000). BJU International, 86(4), 439–447.
- Cicero, A. F. G., et al. (2016). Advances in Therapy, 33(5), 740–754.
- Klippel, K. F., et al. (2017). Lipids in Health and Disease, 16(1), 151.
- Racette, S. B., et al. (2010). American Journal of Clinical Nutrition, 91(1), 32–38.